
Abstract
Early in the COVID-19 pandemic, anecdotal reports emerged suggesting non-steroidal anti-inflammatory drugs (NSAIDs) may increase susceptibility to infection and adversely impact clinical outcomes. This narrative literature review (March 2020–July 2021) attempted to clarify the relationship between NSAID use and COVID-19 outcomes related to disease susceptibility or severity. Twenty-four relevant publications (covering 25 studies) reporting original research data were identified; all were observational cohort studies, and eight were described as retrospective. Overall, these studies are consistent in showing that NSAIDs neither increase the likelihood of SARS-CoV-2 infection nor worsen outcomes in patients with COVID-19. This is reflected in current recommendations from major public health authorities across the world, which support NSAID use for analgesic or antipyretic treatment during COVID-19. Thus, there is no basis on which to restrict or prohibit use of these drugs by consumers or patients to manage their health conditions and symptoms during the pandemic.
Similar content being viewed by others

Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was identified as the cause of coronavirus disease 2019 (COVID-19) in January 20201. Soon afterwards (on March 11, 2020), the World Health Organization (WHO) declared the disease a pandemic2. It has been estimated that around 35% of COVID-19 infections are asymptomatic3. In symptomatic cases, clinical manifestations include fever, cough, body aches and pains, headache, sore throat, gastrointestinal symptoms, acute respiratory disease, pneumonia, and loss of smell or taste4,5,6. Symptoms range in severity from mild to extremely severe, and patients with severe symptoms may require hospitalization and ventilation. In July 2021, the total number of global deaths related to COVID-19 had almost reached 4 million7. Global data on hospitalization rates are lacking but, in the USA between February 2020 and March 2021, there were an estimated 97.1 million symptomatic illnesses and 5.6 million hospitalizations related to COVID-198. In the early stages of the pandemic, best practice for managing hospitalized patients was undefined. Since then, treatment guidelines have been developed that include recommendations on the use of medications known to be beneficial9,10,11,12.
Non-steroidal anti-inflammatory drugs (NSAIDs) were among the medications used in the early stages/phase of the pandemic to manage COVID-19 in both the inpatient and outpatient settings. NSAIDs have diverse structural and pharmacodynamic profiles, but similar modes of action. Their main pharmacological action is inhibition of cyclooxygenase (COX), also known as prostaglandin endoperoxide H synthase13. These drugs are commonly used for their analgesic, anti-inflammatory, or antipyretic effect, and were, therefore, considered as primary candidates for treating a number of the symptoms of COVID-19 (i.e., fever, body aches, headache). Despite this, there were early, unconfirmed, anecdotal reports that NSAIDs could increase susceptibility to infection or aggravate the disease14,15,16. On March 14, 2020, the French Health Minister addressed this topic in a tweet17. Based on limited preclinical data, it was hypothesized that NSAIDs (particularly ibuprofen, which is available worldwide over the counter [OTC] and the most commonly used NSAID) may be detrimental to patients with COVID-19 due to upregulation of angiotensin-converting enzyme (ACE) 2 expression, which, in turn, may facilitate viral entry into host cells and enhance pathogenicity of the viral load14,18. This concern was reported in the British Medical Journal, and despite a lack of evidence to confirm such risk, there was a significant reduction in NSAID use at a time when they could have benefitted those infected with COVID-1919,20,21. In England, the National Health Service suggested that, in the absence of clear evidence, patients should be advised to take paracetamol to treat the symptoms of COVID-19 in preference to NSAIDs22. Around the same time, the lack of scientific data to support an increased risk of SARS-CoV-2 infection or COVID-19 severity with ibuprofen was acknowledged by other authorities, including the European Medicines Agency (EMA)15,22,23.
The potential for NSAIDs to adversely affect the occurrence or severity of COVID-19 via upregulated expression of ACE-2 has been disputed, with several studies reporting that previous and concurrent use of ACE inhibitors or angiotensin receptor blockers, which are widely known to cause upregulated expression of ACE-2, has no impact on COVID-19 frequency or severity24,25,26,27. Recent experimental data suggest that NSAIDs do not affect ACE-2 expression or viral entry into host cells in humans and mice28. Instead, the key effects of NSAIDs appear attributable to the modulation of the inflammatory and humoral immune responses to SARS-CoV-2, as shown in mice studies where NSAIDs limit the production of proinflammatory cytokines and may reduce levels of neutralizing antibodies28. Investigation of this effect in humans, and whether the timing of NSAID use affects COVID-19 pathogenesis, is an important area for further research28.
To clarify the relationship between NSAID use and outcomes relating to COVID-19, we performed a comprehensive review of the published literature evaluating associations between NSAID use and COVID-19 outcomes related to disease susceptibility or severity.
Literature searches
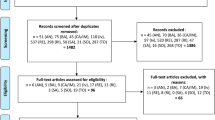
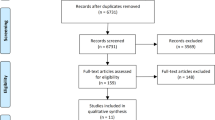
Literature searches were carried out to identify clinical studies, case reports, or review articles relating to the potential effects of NSAIDs on clinical outcomes in human patients with COVID-19 or similar SARS-related coronaviruses. The literature search covered the period from March 2020 to July 2021. The following search string was used to search Embase and Medline:
(“COVID 19”/exp OR “COVID-19” OR “SARS-related coronavirus”/exp OR “SARS-related coronavirus” OR “severe acute respiratory syndrome”/exp OR “severe acute respiratory syndrome”) AND (“ibuprofen”/exp OR ibuprofen or NSAID)) AND (“case report”/de OR “clinical article”/de OR “clinical trial”/de OR “human”/de).
The articles retrieved from the two databases were independently reviewed for relevance by three reviewers. All primary research articles presenting clinical or pharmacoepidemiologic data on NSAID use in the context of COVID-19 were included. Data on outcomes, study population, type of NSAID and dose regimen, and statistical methodology were extracted. Relevant review articles were also checked for additional studies not identified by the literature search.
Results
In total, 24 relevant publications (covering 25 studies) reporting original research data were identified (Table 1). All of these were observational cohort studies, and eight were described as retrospective. No randomized controlled trials were identified. Nineteen of the studies were conducted in patients with COVID-19 or SARS-CoV-2 infection, and the number of participants ranged from 103 to 2.74 million. In addition, a meta-analysis that included 2414 patients from three studies was retrieved29.
NSAIDs—general
A total of 17 publications (covering 18 studies) reported data on the effects of treatment with one or multiple NSAIDs, either prescribed or self-obtained OTC, on outcomes relating to COVID-19. Three of these compared the risks of contracting COVID-19 among individuals treated with NSAIDs with those not receiving NSAIDs. In a cross-sectional study of patients (n = 2102, n = 318 classified as chronic NSAID users) treated at the outpatient Rheumatology Service of Hospital del Mar, Barcelona, Spain, there was no association between the COVID-19 infection rate and chronic NSAID use30. Drew et al. analyzed data from 2.74 million users of the COVID Symptom Study smartphone application from the US, UK, and Sweden31. Initial analysis included 8966 COVID-19-positive test results documented over >60 million person-days of follow-up, and NSAID use was associated with a modest increase in the risk of testing positive for COVID-19 (hazard ratio [HR] 1.22 [95% confidence interval (CI) 1.13–1.32]). However, after adjusting for potential confounders (lifestyle factors, comorbidities, and baseline symptoms), NSAID use was not associated with any change in this risk (HR 1.02 [95% CI 0.94–1.10]). Chandan et al. used a large UK primary care data set (n ≥ 25,000 adults with osteoarthritis) to compare susceptibility to developing suspected or confirmed COVID-19 among patients prescribed NSAIDs vs. other common analgesics (either paracetamol/codeine or paracetamol/dihydrocodeine)32. They found no increase in the risk of suspected/confirmed COVID-19, and no increase in all-cause mortality, among those who were prescribed NSAIDs compared with those who received the comparator drugs.
Two large English cohort studies assessing NSAID use and deaths from COVID-19 (in the general population and patients with rheumatoid arthritis or osteoarthritis) were reported in a single publication33. In the general population (2.5 million participants), prescribed NSAID use did not affect the risk of COVID-related death. Among 1.7 million patients with rheumatoid arthritis or osteoarthritis, analysis with adjustment for confounders showed a lower risk of death from COVID-19 among users of prescribed NSAIDs (HR 0.78 [95% CI 0.64–0.94]). A small cohort study from South Korea (n = 103 adult patients with COVID-19) evaluated factors that increase the COVID-19 patient death rate and showed no statistically significant difference in NSAID use between the survivor and non-survivor COVID-19 patients34.
Three studies investigated the relationship between hospitalization for COVID-19 and NSAID use. In an analysis of the German national registry of patients with inflammatory rheumatic and musculoskeletal disease, NSAID treatment was not identified as a risk factor for COVID-19 related hospitalization35. NSAID therapy was reported in 19.1% of hospitalized patients and 25.4% of non-hospitalized population; univariate analysis indicated that NSAID use had no significant effect on the risk of COVID-19 related hospitalization. Similarly, a European international study of rheumatic disease patients with COVID-19 showed that NSAID therapy was less common in a hospitalized vs. non-hospitalized population (16% vs. 25%)36. A retrospective cohort study of electronic health records for >4500 US patients with COVID-19 did, however, find a statistically significant association between NSAID use and hospitalization37.
A prospective cohort study reported by Abu Esba et al. assessed the association between NSAID use and COVID-19 outcomes (including death, hospital admission, severity, time to clinical improvement, oxygen requirement, and length of hospital stay) in Saudi Arabian adult patients38. The study concluded that acute or chronic use of NSAIDs was not associated with worse COVID-19 outcomes compared to non-NSAID users. A Danish nationwide cohort study also assessed the association between NSAID use (defined as a filled prescription up to 30 days before the patient had a positive test for SARS-CoV-2) and various COVID-19 outcomes39. Treatment with NSAIDs was not associated with 30-day mortality, risk of hospitalization, intensive care unit (ICU) admission, mechanical ventilation, or renal replacement therapy. In addition, a retrospective, multi-center cohort study conducted in the US (n = 1305 patients with COVID-19) showed that NSAID use prior to admission was not associated with development of renal failure or increased mortality40. Indeed, patients using NSAIDs prior to hospitalization had lower odds of mortality (odds ratio [OR]: 0.55 [95% CI 0.39–0.78]), a finding which remained present on multivariate regression analysis (adjusted OR 0.56 [95% CI 0.40–0.82]). In a retrospective South Korean study, Park et al. conducted propensity score-matched analysis to compare outcomes in COVID-19 patients treated with NSAIDs vs. those receiving paracetamol41. No significant differences between the two groups were observed in all-cause mortality or the incidence of ventilator care.
The largest study of COVID-19 patients identified was a US retrospective cohort study using electronic health record data from >250,000 patients42. Potential associations between eight COX inhibitors (paracetamol, aspirin, celecoxib, diclofenac, ibuprofen, ketorolac, meloxicam, naproxen) and COVID-19 severity were assessed. The study reported an association with increased COVID-19 severity for five of the eight agents tested (aspirin, ibuprofen, ketorolac, naproxen, and paracetamol); no significant associations were found for diclofenac, meloxicam, and celecoxib, which display selectivity for inhibition of COX-2. Aspirin and paracetamol (the latter of which is not considered to be COX-selective) were also associated with increased mortality.
A multi-center, observational study conducted in the UK examined the association between use of NSAIDs and outcomes in hospitalized patients (n = 1222) with COVID-19 admitted to eight UK hospitals34,43,44,45. Univariate analysis suggested a modest benefit of prior NSAID use, while multivariable analyses indicated no association between prior NSAID use and time to mortality or length of hospital stay. Another UK study enrolled 78,674 patients across 255 healthcare facilities to assess whether pre-existing NSAID use (within the 2 weeks before hospital admission) was associated with increased severity of COVID-19 disease34,43,44,45. The primary outcome was in-hospital mortality, and secondary outcomes included disease severity at presentation, admission to critical care, receipt of invasive ventilation, receipt of non-invasive ventilation, use of supplementary oxygen, and acute kidney injury. After adjusting for explanatory variables, NSAID use was not associated with worsening of any COVID-19 disease outcomes. A South Korean study of 1824 patients hospitalized with COVID-19 reported higher risk of two composite adverse outcomes among NSAID users (individuals prescribed NSAIDs during the 7 days before hospitalization)46. For the first outcome (in-hospital death, ICU admission, mechanical ventilation use, or sepsis), the adjusted OR was 1.54 (95% CI 1.11–2.15) and, for the second outcome (cardiovascular or renal complications), it was 2.64 (95% CI 1.67–4.16).
A meta-analysis by Kow and Hasan included data from 2414 patients across three studies that compared COVID-19 patients who were users or non-users of NSAIDs29. A pooled HR of 0.86 (95% CI 0.49–1.51) demonstrated no significant difference in the risk of fatality between NSAID users and non-NSAID users.
Ibuprofen
The two large cohort studies by Wong et al. also reported data specifically for ibuprofen33; in both, the general population and patients with rheumatoid arthritis or osteoarthritis, risk of death from COVID-19 was not significantly different between users of ibuprofen vs. other NSAIDs.
Several other studies have assessed the impact of ibuprofen use on the risk of severe COVID-19. A retrospective, single-center study from Israel assessed whether ibuprofen use in individuals with COVID-19 (n = 403) was associated with more severe disease, compared with use of paracetamol or no antipyretics47. Among the entire cohort, 44 patients (11%) needed respiratory support and 12 (3%) died; there was no significant difference in either outcome between the ibuprofen and non-ibuprofen groups, nor between ibuprofen users and exclusive paracetamol users. Kragholm et al. conducted a nationwide register-based study of patients in Denmark with COVID-19 to assess if prescription of ibuprofen affected the risk of severe disease48. The outcome assessed was a 30-day composite of severe COVID-19 diagnosis with acute respiratory syndrome, ICU admission, or death. The study found that there was no significant (p = 0.74) association between ibuprofen prescription claims and severe COVID-19; standardized absolute risks of the composite outcome for ibuprofen-prescribed vs. non-ibuprofen patients were 16.3% (95% CI 12.1–20.6) vs. 17.0% (95% CI 16.0–18.1). Similarly, in the Saudi Arabian study of COVID-19 patients reported by Abu Esba et al., acute use of ibuprofen was not associated with worse COVID-19 outcomes compared to non-NSAID users38.
Castro et al. used electronic health records to identify commonly prescribed medications that may be associated with a lower risk of morbidity among patients with COVID-1949. Records of 12,818 individuals from five US hospitals were assessed. Ibuprofen was associated with favorable outcomes, with users less likely to require hospitalization; among hospitalized patients, use of ibuprofen was associated with a lower risk of ICU admission and mortality.
A study of South Korean patients hospitalized with early-stage COVID-19 (n = 293) reported an increased likelihood of ibuprofen use among individuals with COVID-19 disease progression compared with those exhibiting improvement/stabilization50. However, after adjustment for confounding variables via propensity score matching, the authors found that ibuprofen was not a risk factor for progression. However, a study of 158 hospitalized patients from a single center in Iran reported a significant (p < 0.001) relationship between history of ibuprofen consumption before COVID-19 and the severity of the disease, as well as the mortality rate of patients with COVID-1951.
Aspirin
Several of the studies identified included data for aspirin, and these specific findings are summarized below. Studies assessing the anti-platelet effects of aspirin in patients with COVID-19 are beyond the focus of the current review.
The large study of smartphone application users from the US, UK, and Sweden also included analysis of aspirin users31. The risk of contracting COVID-19 in this group was not significantly different from that among individuals not taking any NSAIDs, either before or after adjustment for confounders (HR after adjustment: 1.03 [95% CI 0.83–1.28]). In a US study of COVID-19 patients admitted to hospital, Chow et al. showed that the use of aspirin was associated with a more favorable disease course52. After adjustment for confounding variables, the risk of ICU admission was reduced by 43% (HR 0.63 [95% CI 0.31–0.90]) in users of aspirin compared with non-users. Similar reductions in the risks of mechanical ventilation (HR 0.56 [95% CI 0.37–0.85]) and in-hospital mortality (HR 0.53 [95% CI 0.31–0.90]) were also observed.
Discussion
NSAIDs are a commonly used class of medication. They are affordable, widely available OTC, and have a well-established benefit-risk profile. NSAIDs provide benefits in managing COVID-19 symptoms, such as fever, body aches, and headache. In addition, many patients with chronic or recurrent inflammatory conditions rely on NSAIDs to manage their everyday symptoms. Therefore, some of these drugs, including ibuprofen, are on the WHO’s list of essential medicines to meet the most important needs in a health system.
Concerns about the potential of NSAID treatment to negatively impact COVID-19 outcomes were raised early in 2020. Since then, robust clinical data have been published, providing the opportunity to define the benefit/risk ratio of NSAID use with an evidence-based approach. The studies identified here represent the best available evidence to inform healthcare professionals and the scientific community. Of the 24 relevant publications identified, the overwhelming majority are consistent in showing that NSAIDs neither increase the likelihood of SARS-CoV-2 infection nor worsen clinical outcomes in patients with COVID-19. In addition, a meta-analysis demonstrated no increase in risk of mortality among NSAID users vs. non-NSAID users29. Another, very recent, systematic review and meta-analysis published after the cut-off of our search found no excess risk of SARS-CoV-2 positivity in patients exposed to NSAIDs15. In addition, in SARS-CoV-2-positive patients, exposure to NSAIDs was not associated with excess risk of hospital admission, death, or severe outcomes.
In contrast to the majority of investigations, four studies reported an association between NSAID use and worse COVID-19 outcomes. In the South Korean study of NSAIDs in hospitalized COVID-19 patients, there were differences in the baseline characteristics of NSAID users and non-users46. NSAID users were older, had more comorbidities, and used more comedications. Although Inverse Probability of Treatment Weighting was used to adjust for such differences, the number of patients exposed to NSAIDs (n = 285) might not have been sufficient to control for multiple confounders, and imbalances in unmeasured parameters such as smoking history or body mass index could have affected the results. Jehi et al. reported an increased risk of hospitalization among NSAID users, although the authors cautioned that their retrospective data did not enable robust conclusions to be drawn and highlighted uncertainty as to whether the observed relationships could have been caused by NSAIDs or underlying comorbidities37. While Samimagham et al. reported a significant relationship between history of ibuprofen consumption before COVID-19 and worse outcomes, the authors commented on the small sample size, focus on hospitalized patients, and lack of information on NSAID dose and indication for use/underlying conditions51. Reese et al. had the benefit of access to electronic health records data from >250,000 patients42. However, this report has not yet been peer reviewed and the authors acknowledge the possibility of incomplete capture of medications taken by the study participants. An update to this article, published in December 2021, accessed >850,000 health records and found no evidence of an association between NSAID use and risk of increasing COVID-19 severity53. Also, detection of significantly worsened disease among users of paracetamol was inconsistent with prior paracetamol studies and inconsistent with the suggestion that paracetamol should be used in preference to NSAIDs such as ibuprofen. While most studies have indicated the use of NSAIDs does not worsen outcomes for COVID-19 patients, the inherent limitations of these observational studies (including the fact that some of them are yet to be peer reviewed) require appropriate consideration when evaluating their results.
A number of review articles and editorials have been published on the possible effects of NSAIDs on the risk or severity of COVID-19. A predominant theme of these publications is the lack of evidence to suggest a mechanism by which NSAIDs (particularly ibuprofen) can worsen outcomes of COVID-19 infection. In fact, the hypothesis involving upregulation of ACE-2 appears to be contradicted by new evidence that NSAIDs do not affect expression of this enzyme28. The importance of basing therapeutic recommendations on robust evidence rather than speculative hypotheses has been emphasized15. The most recent editorial we identified, published in May 2021, concluded “NSAID use with COVID-19 appears to confer no increased risk of poorer outcomes”54.
To further increase complexity, recent data show genetic variations of cytochrome P450 liver oxidative enzyme systems can influence the metabolism of NSAIDs, potentially affecting their elimination from the body, their tissue concentrations, and the greater risks of adverse events19. Genetic variations differ between ethnic groups, meaning, for example, that the risk of higher-than-expected plasma drug levels may be greater in some populations than others. Future implementation of pharmacogenomics into clinical practice could, therefore, help optimize the use of NSAIDs in all patients including those with COVID-19.
Social media is a major influence in healthcare today, including the use of NSAIDs in COVID-19. There is a reasonable possibility of patients’ opinions being affected by information that is not scientifically founded55,56. At every opportunity, the importance of basing treatment decisions on consultation with healthcare professionals rather than unfounded information on social media should be emphasized.
Since the start of the pandemic, major health authorities across the world have published updated guidelines on clinical management of COVID-19 in an effort to combat misinformation. They consistently support the use of NSAIDs for treatment of COVID-19 symptoms, on the basis that there is no evidence of these drugs contributing to worsened outcomes. The WHO published its latest guidance in January 202112. This document recommends that patients with mild COVID-19 “be given symptomatic treatment such as antipyretics for fever and pain, adequate nutrition and appropriate rehydration”, and states “at present, there is no evidence to indicate that there are severe adverse events in patients with COVID-19 as a result of NSAIDs”. On its website, the US Centers for Disease Control and Prevention (CDC) provides information specifically on COVID-19. In the section for healthcare professionals, the question “Do NSAIDs worsen the course of disease for people with COVID-19?” is addressed. In June 2021, the text stated “CDC is currently not aware of any evidence establishing a link between NSAIDs and worsening of COVID-19” and that they were continuing to monitor the situation57. On March 19, 2020, the US Food and Drug Administration (FDA) wrote they were “not aware of any scientific evidence connecting the use of NSAIDs with worsening of COVID-19 symptoms”58. They also reminded readers of the following warning: “the pharmacological activity of NSAIDs in reducing inflammation, and possibly fever, may diminish the utility of diagnostic signs in detecting infections”.
Advice from the EMA, UK National Institute for Health and Care Excellence, and the Australian Therapeutic Goods Administration is similar to that from the FDA, in that it has not been updated since March–May 2020. All these organizations stated that there was no scientific evidence supporting a link between NSAIDs and a worsening of COVID-19 and advocated continued use of NSAIDs as per the approved product information59,60,61. The Singapore Ministry of Health has also conducted a review and concluded that “there is no evidence suggesting additional harms with ibuprofen compared to paracetamol when used to manage symptoms of upper respiratory tract infections”62. Provisional recommendations from the European Alliance of Associations for Rheumatology on the management of rheumatic disease during the pandemic, dated May 2020, stated that NSAID treatment should be continued in patients without COVID-1963. This group also wrote that, based on current knowledge, NSAIDs could be used during the pandemic without additional risk. Similar guidance was published by the American College of Rheumatology (ACR) in December 2020, recommending that NSAID treatment should be continued in patients with or without exposure to SARS-CoV-264. The ACR also stated that possible associations between NSAID use and worse COVID-19 outcomes are yet to be substantiated.
There are several potential limitations to this literature review. This was a narrative literature review, and systematic principles were therefore not followed. As part of the review, the risk of bias in the included studies was not assessed. In addition, the published studies vary considerably in several ways, including geographical setting, medical setting (hospitalized patients, outpatients, primary care), number of patients included, medications and doses (e.g., prescription and OTC doses), outcomes assessed, and statistical methods applied. However, these differences add strength by ensuring the data provide insight from multiple different perspectives. In particular, studies have been identified from multiple regions of the world, providing a global aspect of the challenge and, importantly, showing the same responses are reported regardless of ethnicity.
In summary, from observational studies conducted to date, there is no evidence of an association between the use of NSAIDs and increased susceptibility to COVID-19 or increased disease severity, and no plausible causative mechanism by which NSAIDs would increase susceptibility to or the severity of COVID-19 illness. This is reflected in the current recommendations from major public health authorities across the world, which support NSAID use for analgesic or antipyretic treatment during COVID-19. Although further data (e.g., from randomized controlled trials) are required to fully elucidate the relationship between NSAID therapy and COVID-19 severity, there is no basis on which to restrict or prohibit use of these drugs by consumers or patients to manage their health conditions and symptoms during the pandemic. As NSAID users often have clinical characteristics associated with worsened outcomes in COVID-19, restricting access or prohibiting use of these drugs during the pandemic may have a negative impact on patients who consequently are likely to use opioids or subtherapeutic treatment options.
Data availability
Data included in the review is all sourced from published information and publicly available.
References
Zheng, J. SARS-CoV-2: an emerging coronavirus that causes a global threat. Int. J. Biol. Sci. 16, 1678–1685 (2020).
World Health Organization. Listings of WHO’s response to COVID-19. https://www.who.int/news/item/29-06-2020-covidtimeline (World Health Organization, 2020).
Almadhi, M. A. et al. The high prevalence of asymptomatic SARS-CoV-2 infection reveals the silent spread of COVID-19. Int. J. Infect. Dis. 105, 656–661 (2021).
World Health Organization. Coronavirus. https://www.who.int/health-topics/coronavirus#tab=tab_3 (World Health Organization, 2021).
Zhang, J. J. et al. Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy 75, 1730–1741 (2020).
Lai, C.-C. et al. Asymptomatic carrier state, acute respiratory disease, and pneumonia due to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2): facts and myths. J. Microbiol. Immunol. Infect. 53, 404–412 (2020).
World Health Organization. WHO Coronavirus (COVID-19) Dashboard. https://covid19.who.int/ (World Health Organization, 2021).
Centers for Disease Control and Prevention. Estimated COVID-19 Burden. https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/burden.html (Centers for Disease Control and Prevention, 2021).
Chalmers, J. D. et al. Management of hospitalised adults with coronavirus disease 2019 (COVID-19): a European Respiratory Society living guideline. Eur. Respir. J. 57, 2100048 (2021).
National Institutes of Health. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. https://www.covid19treatmentguidelines.nih.gov/ (National Institutes of Health, 2021).
Sodum, N., Kumar, G., Rao, V., Kumar, N. & Rao, C. M. Treatment approaches for COVID-19: a critical review. Mini. Rev. Med. Chem. [Online ahead of print] (2021).
World Health Organization. The Use of Non-steroidal Anti-inflammatory Drugs (NSAIDs) in Patients with COVID-19. https://apps.who.int/iris/bitstream/handle/10665/331796/WHO-2019-nCoV-Sci_Brief-NSAIDs-2020.1-eng.pdf (World Health Organization, 2020).
Ghlichloo, I. & Gerriets, V. Nonsteroidal anti-inflammatory drugs (NSAIDs). in StatPearls (Treasure Island (FL), 2021).
Fang, L., Karakiulakis, G. & Roth, M. Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? Lancet Respir. Med. 8, e21 (2020).
Moore, N., Carleton, B., Blin, P., Bosco-Levy, P. & Droz, C. NSAIDs and COVID-19: a systematic review and meta-analysis. Drug. Saf. 44, 929–938 (2021).
Vosu, J. et al. Is the risk of ibuprofen or other non-steroidal anti-inflammatory drugs increased in COVID-19? J. Paediatr. Child. Health 56, 1645–1646 (2020).
Véran, O. [Tweet] Re: COVID-19. https://twitter.com/olivierveran/status/1238776545398923264?lang=en (2020).
Hoffmann, M. et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell 181, 271–280.e278 (2020).
Almarzooq, A. A. Exploration of interethnic variation in the ibuprofen metabolizing enzyme CYP2C9: a genetic-based cautionary guide for treatment of COVID-19 symptoms. medRxiv. https://doi.org/10.1101/2021.01.09.21249508 (2021).
Little, P. Non-steroidal anti-inflammatory drugs and covid-19. BMJ 368, m1185 (2020).
Day, M. Covid-19: ibuprofen should not be used for managing symptoms, say doctors and scientists. BMJ 368, m1086 (2020).
National Health Service England. Novel Coronavirus—Anti-inflammatory Medications. https://www.cas.mhra.gov.uk/ViewandAcknowledgment/ViewAlert.aspx?AlertID=103001 (National Health Service England, 2020).
Day, M. Covid-19: European drugs agency to review safety of ibuprofen. BMJ 368, m1168 (2020).
Kuster, G. M. et al. SARS-CoV2: should inhibitors of the renin-angiotensin system be withdrawn in patients with COVID-19? Eur. Heart J. 41, 1801–1803 (2020).
Mancia, G., Rea, F., Ludergnani, M., Apolone, G. & Corrao, G. Renin-angiotensin-aldosterone system blockers and the risk of Covid-19. N. Engl. J. Med. 382, 2431–2440 (2020).
Reynolds, H. R. et al. Renin-angiotensin-aldosterone system inhibitors and risk of Covid-19. N. Engl. J. Med. 382, 2441–2448 (2020).
Trifirò, G., Crisafulli, S., Andò, G., Racagni, G. & Drago, F. Should patients receiving ACE inhibitors or angiotensin receptor blockers be switched to other antihypertensive drugs to prevent or improve prognosis of novel coronavirus disease 2019 (COVID-19)? Drug. Saf. 43, 507–509 (2020).
Chen, J. S. et al. Non-steroidal anti-inflammatory drugs dampen the cytokine and antibody response to SARS-CoV-2 infection. J. Virol. 95, e00014–21 (2021).
Kow, C. S. & Hasan, S. S. The risk of mortality in patients with COVID-19 with pre-diagnosis use of NSAIDs: a meta-analysis. Inflammopharmacology 29, 641–644 (2021).
Blanch-Rubió, J. et al. Influence of anti-osteoporosis treatments on the incidence of COVID-19 in patients with non-inflammatory rheumatic conditions. Aging 12, 19923–19937 (2020).
Drew, D. A. et al. Aspirin and NSAID use and the risk of COVID-19. medRxiv. https://doi.org/10.1101/2021.04.28.21256261 (2021).
Chandan, J. S. et al. Nonsteroidal antiinflammatory drugs and susceptibility to COVID-19. Arthritis Rheumatol. 73, 731–739 (2021).
Wong, A. Y. et al. Use of non-steroidal anti-inflammatory drugs and risk of death from COVID-19: an OpenSAFELY cohort analysis based on two cohorts. Ann. Rheum. Dis. 80, 943–951 (2021).
Hwang, J. M., Kim, J. H., Park, J. S., Chang, M. C. & Park, D. Neurological diseases as mortality predictive factors for patients with COVID-19: a retrospective cohort study. Neurol. Sci. 41, 2317–2324 (2020).
Hasseli, R. et al. Older age, comorbidity, glucocorticoid use and disease activity are risk factors for COVID-19 hospitalisation in patients with inflammatory rheumatic and musculoskeletal diseases. RMD. Open. 7, e001464 (2021).
Gianfrancesco, M. et al. Characteristics associated with hospitalisation for COVID-19 in people with rheumatic disease: data from the COVID-19 Global Rheumatology Alliance physician-reported registry. Ann. Rheum. Dis. 79, 859–866 (2020).
Jehi, L. et al. Development and validation of a model for individualized prediction of hospitalization risk in 4,536 patients with COVID-19. PLoS ONE 15, e0237419 (2020).
Abu Esba, L. C. et al. Ibuprofen and NSAID use in COVID-19 infected patients is not associated with worse outcomes: a prospective cohort study. Infect. Dis. Ther. 10, 253–268 (2021).
Lund, L. C. et al. Adverse outcomes and mortality in users of non-steroidal anti-inflammatory drugs who tested positive for SARS-CoV-2: a Danish nationwide cohort study. PLoS Med. 17, e1003308 (2020).
Imam, Z. et al. Older age and comorbidity are independent mortality predictors in a large cohort of 1305 COVID-19 patients in Michigan, United States. J. Intern. Med. 288, 469–476 (2020).
Park, J., Lee, S. H., You, S. C., Kim, J. & Yang, K. Non-steroidal anti-inflammatory agent use may not be associated with mortality of coronavirus disease 19. Sci. Rep. 11, 5087 (2021).
Reese, J. T. et al. Cyclooxygenase inhibitor use is associated with increased COVID-19 severity. medRxiv. https://doi.org/10.1101/2021.04.13.21255438 (2021).
Bruce, E. et al. Prior routine use of non-steroidal anti-inflammatory drugs (NSAIDs) and important outcomes in hospitalised patients with COVID-19. J. Clin. Med. 9, 2586 (2020).
Drake, T. M. et al. Non-steroidal anti-inflammatory drug use and outcomes of COVID-19 in the ISARIC Clinical Characterisation Protocol UK cohort: a matched, prospective cohort study. Lancet Rheumatol. 3, e498–e506 (2021).
Perkins, S. J. et al. 41 Clinical outcomes among COVID-19 patients taking non-steroidal anti-inflammatory drugs. Ann. Emerg. Med. 76, S17–S17 (2020).
Jeong, H. E. et al. Association between nonsteroidal antiinflammatory drug use and adverse clinical outcomes among adults hospitalized with coronavirus 2019 in South Korea: a nationwide study. Clin. Infect. Dis. 73, e4179–e4188 (2021).
Rinott, E., Kozer, E., Shapira, Y., Bar-Haim, A. & Youngster, I. Ibuprofen use and clinical outcomes in COVID-19 patients. Clin. Microbiol Infect. 26, 1259.e5–1259.e7 (2020).
Kragholm, K. et al. Association between prescribed ibuprofen and severe COVID-19 infection: a nationwide register-based cohort study. Clin. Transl. Sci. 13, 1103–1107 (2020).
Castro, V. M., Ross, R. A., McBride, S. M. & Perlis, R. H. Brief report: identifying common pharmacotherapies associated with reduced COVID-19 morbidity using electronic health records. medRxiv. https://doi.org/10.1101/2020.04.11.20061994 (2020).
Choi, M. H. et al. Clinical characteristics and disease progression in early-stage COVID-19 patients in South Korea. J. Clin. Med. 9, 1959 (2020).
Samimagham, H. R., Arabi, M., Hooshyar, D. & KazemiJahromi, M. The association of non-steroidal anti-inflammatory drugs with COVID-19 severity and mortality. Arch. Clin. Infect. Dis. 15, e106847 (2020).
Chow, J. H. et al. Aspirin use is associated with decreased mechanical ventilation, intensive care unit admission, and in-hospital mortality in hospitalized patients with coronavirus disease 2019. Anesth. Analg. 132, 930–941 (2021).
Reese, J. T. et al. NSAID use and clinical outcomes in COVID-19 patients: a 38-center retrospective cohort study. medRxiv. https://doi.org/10.1101/2021.04.13.21255438 (2021).
Kragholm, K., Torp-Pedersen, C. & Fosbol, E. Non-steroidal anti-inflammatory drug use in COVID-19. Lancet Rheumatol. 3, e465–e466 (2021).
Arca, K. N. et al. COVID-19 and headache medicine: a narrative review of non-steroidal anti-inflammatory drug (NSAID) and corticosteroid use. Headache 60, 1558–1568 (2020).
Kakodkar, P., Kaka, N. & Baig, M. N. A comprehensive literature review on the clinical presentation, and management of the pandemic coronavirus disease 2019 (COVID-19). Cureus 12, e7560 (2020).
Centers for Disease Control and Prevention. Clinical Questions About COVID-19: Questions and Answers. https://www.cdc.gov/coronavirus/2019-ncov/hcp/faq.html#Drugs-and-Investigational-Therapies (Centers for Disease Control and Prevention, 2021).
Food and Drug Administration. FDA Advises Patients on Use of Non-steroidal Anti-inflammatory Drugs (NSAIDs) for COVID-19. https://www.fda.gov/drugs/drug-safety-and-availability/fda-advises-patients-use-non-steroidal-anti-inflammatory-drugs-nsaids-covid-19 (Food and Drug Administration, 2020).
European Medicines Agency. EMA Gives Advice on the Use of Non-steroidal Anti-inflammatories for COVID-19. https://www.ema.europa.eu/en/news/ema-gives-advice-use-non-steroidal-anti-inflammatories-covid-19 (European Medicines Agency, 2020).
National Institute for Health and Care Excellence. COVID-19 Rapid Evidence Summary: Long-term Use of Non-steroidal Anti-inflammatory Drugs (NSAIDs) for People with or at Risk of COVID-19. https://www.nice.org.uk/advice/es25/chapter/Key-messages (National Institute for Health and Care Excellence, 2020).
Therapeutic Goods Administration. No Evidence to Support Claims Ibuprofen Worsens COVID-19 Symptoms. https://www.tga.gov.au/alert/no-evidence-support-claims-ibuprofen-worsens-covid-19-symptoms (Therapeutic Goods Administration, 2020).
Singapore Ministry of Health. Should Ibuprofen be Used for COVID-19? https://www.moh.gov.sg/docs/librariesprovider5/clinical-evidence-summaries/ibuprofen-for-covid-19-(updated-3-june-2020)347054f94340416f93e2fe2aca41918b.pdf (Singapore Ministry of Health, 2020).
Landewe, R. B. et al. EULAR provisional recommendations for the management of rheumatic and musculoskeletal diseases in the context of SARS-CoV-2. Ann. Rheum. Dis. 79, 851–858 (2020).
Mikuls, T. R. et al. American College of Rheumatology Guidance for the management of rheumatic disease in adult patients during the COVID-19 pandemic: version 3. Arthritis Rheumatol. 73, e1–e12 (2021).
Acknowledgements
Medical writing support was provided by Tony Reardon of Spirit Medical Communications Ltd (Manchester, UK). Funding for this support was provided by GSK.
Author information
Authors and Affiliations
Contributions
A.K., A.L.H., and V.Z. conducted the literature searches and analyzed search results for relevant articles to include. All authors contributed to drafting and critical review of the manuscript content. All authors approved the final version of the manuscript for submission.
Corresponding author
Ethics declarations
Competing interests
P.K. is a speaker and an advisory board member for GSK. B.H.M. is an advisor to Lilly, Scilex, and Averitas, a member of the Speaker’s Bureau for Adapt and Scilex, and holds stocks in Johnson & Johnson. L.G. is a member of the French board of GRAINS, which is supported by GSK. A.K., A.L.H., V.Z., R.P., and S.B. are current or former employees of GSK Consumer Healthcare.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kushner, P., McCarberg, B.H., Grange, L. et al. The use of non-steroidal anti-inflammatory drugs (NSAIDs) in COVID-19. npj Prim. Care Respir. Med. 32, 35 (2022). https://doi.org/10.1038/s41533-022-00300-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41533-022-00300-z
This article is cited by
-
The impact of perioperative nonsteroidal anti-inflammatory drugs on the postoperative outcomes of spinal surgery: a meta-analysis of 23 randomized controlled trials
Neurosurgical Review (2024)
-
What are the current anti-COVID-19 drugs? From traditional to smart molecular mechanisms
Virology Journal (2023)
-
Development of Delayed-Release Pellets of Ibuprofen Using Kollicoat® MAE 100P via Hot-Melt Extrusion Technology
Journal of Pharmaceutical Innovation (2023)
-
Pediatric Pericarditis: Update
Current Cardiology Reports (2023)
-
Ibuprofen, other NSAIDs and COVID-19: a narrative review
Inflammopharmacology (2023)
